Reviews
User Score
Rate This
Descriptions:
The 9 steps to establish a CV of the MPO are as follows:
1. Identify and dissect the pubic tubercle across the midline and Cooper ligament (CL). For large, direct hernias, extend the dissection to the contralateral CL
.2. Rule out a direct hernia. Visualize anatomy through the inflated balloon during totally extraperitoneal and extended totally extraperitoneal repairs to detect a direct hernia before dissection. Remove unusual fat in the Hasselbach triangle.
3. Dissect at least 2 cm between CL and the bladder to facilitate flatplacement of the medial and inferior edge of mesh toward thespace of Retzius, thereby avoiding mesh displacement caused by bladder distention.
4. Dissect between CL and the iliac vein to identify the femoralorifice and rule out a femoral hernia.
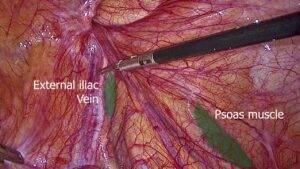
5. Dissect the indirect sac and peritoneum sufficiently to parietalize the cord’s elements. This step is often not completed, especially in a small surgical field. To ensure compliance with this requirement, continue to dissect until the cord’s elements lie flat. Then, visualize the psoas muscle and iliac vessels, pull the sac and peritoneum upward without triggering the movement of the cord’s elements, and dissect between the cord’s elements to avoid missing a tail of the sac.
6. Identify and reduce cord lipomas (which may appear small and unimportant until reduced). Usually lateral to the cord’s elements, they should not be confused with lymph nodes(which are generally spared). Most lipomas do not require removal, but should be placed above the mesh to help prevent mesh rolling upward.
7. Dissect peritoneum lateral to the cord’s elements laterally beyond the anterosuperior iliac spine (ASIS), sweeping it back inferiorly well behind the mesh’s inferior border.
8. Perform the dissection, provide mesh coverage, and ensure that mesh and mechanical fixation are placed well above an imaginary-inter-ASIS line and any defects, thereby avoiding recurrence and nerve injury, especially to the ilioinguinal nerve.
9. Place the mesh only when items 1 to 8 are completed and hemostasis has been verified. Mesh size should be at least 15 X 10 cm, although a larger piece of mesh is sometimes required to cover the MPO. Preferably, choose mesh that adapts to the contour of the space and the cord’s elements. It should not have undue memory. Place it without creases or folds. Avoid splitting the mesh. Ensure that its lateroinferior corner lies deep against the wall and does not roll up during space deflation (use glue or careful suturing if necessary).
Analysis of Video
Presenter: Herniacademia
Organization: Herniacademia
Video Source: Herniacademia
Video Link: https://www.youtube.com/watch?v=sBGfvUCiioc
Year of Posting: 2021
Case Details: Not Available
Type of Video: Edited
Duration: 3.39 minutes
Step of Surgery: Well written
Audio commentary: No
Questions & Answers: No
Watch More Videos: Laparoscopic Anatomy of Inguinal Hernia: Static view